Millions of Americans may be receiving inadequate cholesterol screening, according to new research highlighting the superiority of apoB testing over conventional LDL cholesterol measurements.
The study demonstrates that apoB, which quantifies the actual number of harmful cholesterol particles in the bloodstream, outperforms standard LDL testing in identifying patients at highest cardiovascular risk. Researchers found that switching to apoB-based screening could prevent more heart attacks and strokes while maintaining cost-effectiveness within the U.S. healthcare system.
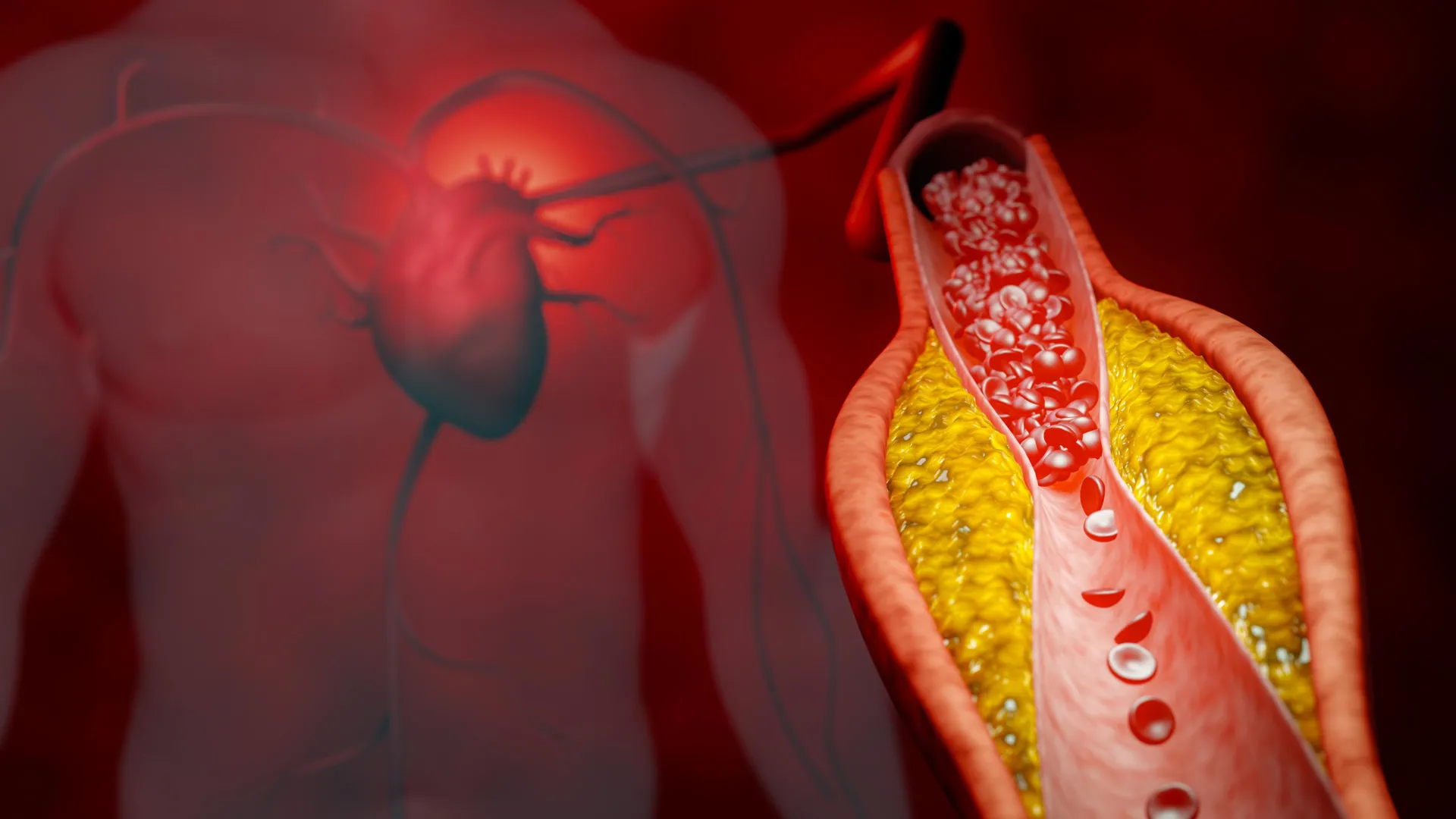
LDL cholesterol tests measure only the concentration of cholesterol within particles, not the particle count itself. A patient can have normal LDL levels yet harbor numerous small, dense LDL particles, each capable of damaging arterial walls. ApoB directly counts these atherogenic particles, providing clinicians with more precise risk stratification.
The research indicates that apoB testing would enable more targeted treatment decisions. Patients with elevated apoB but normal LDL levels would receive appropriate intensified therapy, preventing unnecessary events. Conversely, some patients with modestly elevated LDL but low particle counts might avoid overtreatment.
The economic analysis proved central to the study's findings. The researchers calculated that despite apoB testing's slightly higher cost per test, the prevention of cardiovascular events generates net savings for the healthcare system. Each prevented heart attack or stroke yields substantial medical cost reductions that exceed testing expenses.
Current guidelines from major cardiology organizations increasingly recognize apoB's clinical value, yet widespread adoption remains limited. Many laboratories continue performing standard lipid panels because of established infrastructure and provider familiarity. Insurance coverage varies, with some plans reimbursing apoB testing only for specific patient populations.
The study underscores a gap between available science and clinical practice. Cardiologists can already order apoB testing, but population-level implementation requires changes in screening protocols, provider education